Many countries turn a blind eye to domestic abuse – but Nepal's approach could be the model for a global solution.
By Tricia Taormina
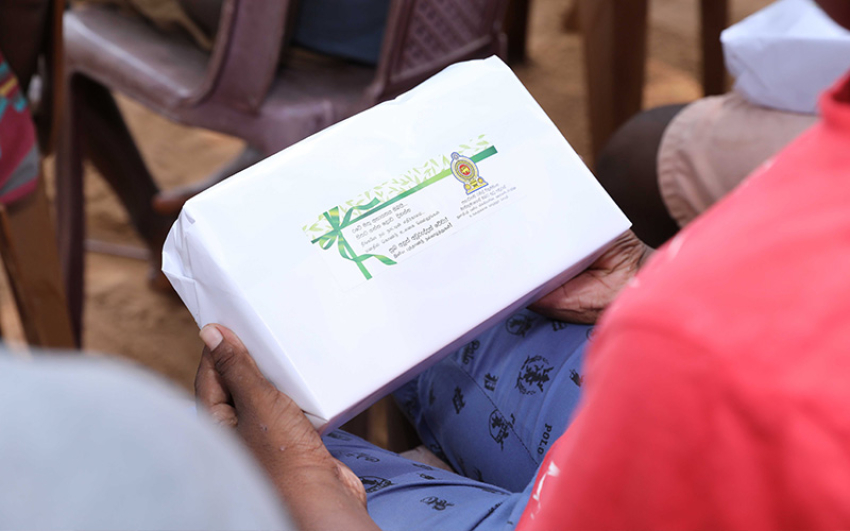
In the crowded emergency ward of a hospital, Dr Prabhat Rijal met a patient covered in bruises.Her visit was expected. The doctors at Rapti Sub-Regional Hospital in Ghorari, western Nepal see at least one case like this a night. It’s usually shortly after dusk, when abusive men come home from work and start drinking. The patients tend to come in gripping their stomachs or complaining of earaches, but the nurses and doctors look out for bruises or cuts on their bodies that suggest a different story.Rijal, suspecting something was off, asked the woman what happened. She had run out of her house after her husband beat her, the patient said. Her hair was still slick with sweat.The team at the crisis management centre – staff nurse Punam Rawat, counsellor Radha Paudel and police officer Sabita Thapa – listens to a patient The dimly lit emergency ward is busy late into the night, with children running around and patients on every gurney, so Rijal and a nurse led the woman into a private room and shut the door. They followed the script they normally employ. Abuse is not normal or inevitable, they told her. She has options.Moments later, the nurse led her to the one-stop crisis centre, a separate wing of the hospital where patients facing abuse can meet counselors and a female police officer.The one-stop crisis management centre at Rapti Sub-Regional Hospital in Ghorahi, Nepal
Intimate partner violence often leads to long-term health problems. And a doctor’s office is usually the first – if not the only – place where someone might not only notice the problem, but have the expertise and authority to help.ritise intervention in healthcare settings. But Nepal, which has some of the highest levels of domestic abuse, is among a growing number of countries embracing a health response – placing support services inside hospitals and training providers to identify and refer abused patients.‘As common as asthma and diabetes’Although intimate partner violence can happen to anyone, it disproportionately affects women.Worldwide, almost one-third of women who have been in a relationship report having experienced physical or sexual violence from their partner. Intimate partner violence is exacerbated in countries experiencing or recovering from conflict, like the Democratic Republic of the Congo and northern Uganda. Although attitudes are changing, studies suggest it is also more accepted in countries across Asia, Africa, and Oceania
In the US, 32% of women have experienced physical partner violence and 16% have experienced sexual violence from a partner It isn’t only the developing world. A third of women in Denmark and just under 30% in the United Kingdom report having experienced intimate partner violence at least once in their lifetime, for example, with around 5% reporting an occurrence in the last 12 months. In the US, 32% of women have experienced physical partner violence and 16% have experienced sexual violence from a partner, with almost 4% experiencing physical violence and 2% experiencing sexual violence in the last year.
The impact violence has on women’s health is immense.
In the US, intimate partner violence results in 2 million injuries each year, making it a larger health problem than obesity and smoking. It is associated with chronic pain, asthma, difficulty sleeping, irritable bowel syndrome, heart disease, diabetes, stroke and sexually transmitted diseases. Women who have experienced violence from a partner are at higher risk for suicide and more likely to suffer from depression, anxiety, panic attacks and post-traumatic stress disorder.
Since 40% of female homicide victims are killed by their intimate partners, intervening at this stage can save lives
Medical workers are often the first service responders to come in contact with people experiencing abuse: in the US, for example, women in abusive relationships visit health centres 2.5 times as often as other patients.
Sabita (not her real name) visits the one-stop crisis centre for follow-up counselling once a month (Credit: Bunu Dhungana)
Since 40% of female homicide victims are killed by their intimate partners, intervening at this stage can save lives. One study of 139 female homicides that took place over five years in Kansas City found that nearly one-quarter of homicides – 34 – were related to domestic violence. And 15 women had presented to an emergency department – 14 of them with injuries – within the two years before they were killed. A recent survey of 1,554 victims attended to by police after domestic violence calls found that 88% reported having survived a previous strangulation attempt.
But health providers are often unprepared to help patients. In Britain, a 2017 study found that most medical trainings don’t adequately cover intimate partner violence. Although the Affordable Care Act in the United States mandates that more insurance plans cover screening and counselling for patients facing violence, the US government still doesn’t have a national protocol.
Counsellor Radha Paudel stands in front of the room where she meets with patients (Credit: Bunu Dhungana)
Training medical workers to identify and refer abused patients depends on how a country funds its healthcare, says Kelsey Hegarty, a family physician and researcher who helps develop health interventions in Australia. Governments can’t require privately funded institutions train their staff on responding to intimate-partner violence and many governments don’t fund protocols and trainings. As a result, civil society groups often take on the task of developing interventions and in-hospital services.
“For something that is as common as asthma and diabetes and causes ill health, it’s very disturbing,” says Hegarty.
Not sensitising health providers has consequences. One recent study suggested that some health providers in Lebanon feel violence is justified if women exhibit aggressive behavior.
Unsurprisingly, patients often don’t feel comfortable disclosing abuse. In Nepal – where nearly half of women have experienced some form of abuse – patients worry that health providers will laugh at them or accuse them of not being “good” wives.
The police didn’t even care when I told them what happened to me before, so why would doctors care? – Neha
“The police didn’t even care when I told them what happened to me before, so why would doctors care?” says Neha, who had been in an abusive marriage before she visited a one-stop crisis centre in Nepal. (To protect the safety of the women interviewed, we have not used real names.)
Neha, 38, waits outside a shelter home and knitting centre for survivors of intimate partner violence (Credit: Bunu Dhungana)
There is debate over how health providers should identify patients like Neha. Some advocates recommend screenings which require that health providers ask patients if they’ve faced abuse. But there’s little evidence to suggest it helps. A review of 11 studies in the British Medical Journal found that screenings helped identify patients facing abuse, but did not necessarily help them access support services. The World Health Organization advises against screenings in its guidelines on gender-based violence for health providers.
Instead, many experts suggest approaches like the one Nepal has embraced.
Nepal's approach
Inside the one-stop crisis centre at the hospital in Ghorahi, Maya was curled up on a teal-covered cot. She had visited the emergency ward a day before. Now, she was back to meet with counsellor Radha Paudel, who sat crouched near her bed, inspecting a string of bruises running up her arm. On a pillow nearby was a sheet of paper listing her other symptoms – a headache, hematoma in her right hand, swelling on her head, pain in her chest and on her upper and lower back.
“You came in earlier with your husband, too,” Radha said in a near-whisper.
“My husband refused to come today,” Maya said. He was at her house watching her children.
Maya, 34, waits in the examination room inside the one-stop crisis centre with her mother and neighbour (Credit: Bunu Dhungana)
Months earlier, Maya had lodged a complaint against her husband, who was briefly arrested, and filed for divorce with the help of Sabita Thapa, the police officer who works at the crisis centre full-time. Radha connected Maya with a local women’s group to help her establish an independent source of income. Her situation reflects an imperfect, but evolving health response. Although Maya still faced abuse, the one-stop crisis centre has linked her to multiple services. Her husband has moved out and their divorce is pending in court.
Nepal opened its first one-stop crisis centre in 2011 in its central and far-western regions and continues to place them in hospitals around the country. In 2015, the government developed a protocol to help health providers identify and refer more patients to the crisis centres, which received technical support from Jhpiego and the UN Population Fund and is now funded by the government.
Hundreds of health providers have been trained so far, ranging from gynaecologists to family physicians at small health posts high in the Himalayas.
In 2013, only 74 women reported abuse to the hospital. By 2017 that figure jumped to 493 women
At the hospital in Ghorahi, experts believe this multi-faceted approach has helped increase the number of women reporting abuse and receiving counselling and legal advice. In 2013, only 74 women reported abuse to the hospital. By 2017 that figure jumped to 493 women. Although most women visited the hospital to report abuse on their own, each year the number of nurses or doctors referring patients to counsellors increases.
“Health workers were scared handling these types of cases,” says Saroja Pande, one of the physicians who helped design the protocol. “They would refer them to services, but the survivors were traumatised and would drop out of follow-ups, stay at home and develop depression. Some killed themselves.”Today’s trainings are comprehensive. They include a mix of theory, games and role-play scenarios, including a courtroom simulation to prepare health providers for what will happen if they are called to present evidence.
Dr Prabhat Rijal meets a patient in the outpatient department; he regularly identifies intimate partner violence cases and refers them to the crisis centre Another goal is to expand empathy. Medical workers are encouraged to recognise and question biases they may hold about abuse. During one session, the trainers ask them if they believe a woman wearing a short skirt is assaulted because of her clothing choice. They take the opportunity to debunk myths about what motivates abusers.
We tell health providers, if you can’t serve a survivor from the bottom of your heart, then don’t touch their case – Ishwor Prasad Upadhyaya
Ishwor Prasad Upadhyaya, the training coordinator, says they want health providers to think of this work as more than a job. “We tell them, if you can’t serve a survivor from the bottom of your heart, then don’t touch their case,” he says.“If you can’t serve them, send them to another health worker.”
Other countries have similar approaches. One-stop crisis models and their variants exist at health centres in Rwanda, Guatemala, India, England, Malaysia, South Africa and Colombia, among others. Jordan’s government has a protocol for health providers and reproductive health clinics, like Profamilia in the Dominican Republic, screen patients for gender-based violence.
But these approaches still face serious challenges. Experts agree that merely training health providers is not enough unless a country has strong support services in place, including shelters. But in Nepal, as in many countries, shelters are underfunded, only let domestic abuse survivors stay for a brief period of time, and can be rare in rural areas.
The counselling room inside the one-stop crisis centre At the hospital in Ghorahi, there can be delays in following up with patients, which may make them less likely to seek support services. Many women also opt for family counselling instead of filing police complaints against their husbands, owing to a lack of family and financial support. Police officers in Nepal often urge mediation as an alternative to prosecution, but research in the United States suggests it can increase risk.
Worldwide, the burnout rate for health providers engaged in this work is also high, says Upala Devi, the gender-based violence coordinator of UNFPA.
“I think what we’re seeing right now in terms of momentum is very positive and welcome,” she says. “But at the same time much more remains to be done.”
How untrained health providers can help
Experts agree that health providers who haven’t been trained can still help identify and refer abused patients.
Hegarty has only one piece of advice: read the World Health Organization’s guidelines on responding to gender-based violence, which outline evidence-based suggestions.
Most importantly, the guidelines list the things a health provider should consider before asking a patient if they face abuse – such as make sure you are in a private setting, ensure confidentiality, follow a protocol, and refer him or her to resources, including legal and other support services.
Ideally, health providers should be trained on how to sensitively ask about abuse. But in situations where this isn’t possible, the guidelines explain how to listen, enquire about needs, and validate the patient’s experiences.
If a patient seems depressed or answers questions erratically, a health provider should consider asking them about their relationships
In Nepal, health providers keep an eye out for patients who come in with vague symptoms or symptoms that don’t correspond with an examination’s physical findings. They also observe their behaviour and that of those accompanying them. If a patient seems depressed or answers questions erratically, a health provider should consider asking them about their relationships or refer them to a qualified counselor, says Pande. If the family member or spouse accompanying the patient refuses to leave her alone with a health provider, this might also signal abuse.
Jinan Usta, a physician who has designed training for health providers in Lebanon, says it’s important to develop safety plans with patients if they choose to stay with their abusers. First, medical providers should ask the patient whether the violence has increased over time or in severity, and if there are firearms or other sharp instruments around. If there are, she recommends patients leave the house immediately when their abuser starts acting violently.
There are a number of other safety measures: avoid hiding in enclosed spaces, have a number on your mobile phone of someone you can call immediately, hide sharp instruments, and keep the front door of your home unlocked so that you can quickly exit.
Usta believes that listening to domestic abuse survivors holds its own power. “It’s enough to listen to the women and make them feel like they are not alone in this,” she says.
Three years ago, Sabita reported abuse here; she regularly refers other women to the centre now (Credit: Bunu Dhungana)
Sabita agrees. On a recent afternoon, she walked into the crisis centre in Ghorahi during a burst of monsoon rain and sat in a corner, watching the staff shuffle papers.
Three years ago, she reported abuse here. Now she stops by for follow-up counselling. She has moved back in with her husband, but says the abuse stopped shortly after the crisis centre staff helped organise his treatment for depression. She regularly refers other women to the crisis centre.
“They treat us better than our mothers and fathers,” she says.
If you have experienced gender-based violence or know someone who you believe has, you can consult the UN Women’s Global Database on Violence Against Women to find a support hotline in your country.
Those who have experienced or witnessed gender-based violence in Nepal can call 1145, a 24-hour toll free helpline run by the National Women Commission that offers psyco-social support, legal aid, and shelter information.
This story is part of the Health Gap, a special series about how men and women experience the medical system – and their own health – in starkly different ways. Do you have an experience to share? Or are you just interested in sharing information about women's health and wellbeing? Join our Facebook group Future Woman and be a part of the conversation about the day-to-day issues that affect women’s lives.
Join 800,000+ Future fans by liking us on Facebook, or follow us on Twitter.
The health risks of maturing early
Many more boys get diagnosed with ADHD than girls. But more girls may have the condition than we think – and their struggle to receive a diagnosis can affect their whole lives.Emily Johnson-Ferguson’s mind has been racing for as long as she can remember. The eating disorders she began suffering from as a teenager were her attempt to slow down her brain. Doctors tried to blame them on family problems and stress, but she knew that wasn’t it.It was only last year, aged 42, that she finally got to the root of her problems: ADHD.Johnson-Ferguson is not alone. Though the stereotypical image of ADHD is a boy bouncing around a classroom, that’s not the whole picture. Girls can have ADHD, too – and many go without diagnosis, and without treatment that could change their lives.ADHD is a neurodevelopmental disorder that comes in three types: inattentive, hyperactive/impulsive, or a combination of both. People with inattention may forget things, struggle to get organised, and find themselves easily distracted. Those with hyperactivity and impulsivity might struggle to stay sitting down, constantly fidget, and interrupt conversations.
Some adults with ADHD rely on multiple reminders and calendars to stay organised The condition is usually first diagnosed in childhood, but most people don’t grow out of it. For those whose symptoms are missed as children, living with undiagnosed ADHD as they move into adulthood causes problems.“When I was left to my own devices at university I just couldn't concentrate at all,” says Johnson-Ferguson. She switched courses, but it didn’t help. Her bulimia persisted throughout university, and for the next 20 years she also used alcohol, caffeine, and sugary drinks to self-medicate – common among adults with ADHD.
As her marriage broke down, she started to find life even more difficult. In an effort to start afresh, Johnson-Ferguson gave up her bad habits, but found no respite from her symptoms; instead, they got worse. At her lowest point she was spending days on end in bed. “At that time I couldn’t focus on anything,” she says.
Attention deficit
There is a concrete difference between the prevalence of ADHD in boys versus girls. In one study of 2,332 twins and siblings, Anne Arnett, a clinical child psychologist at the University of Washington, found that a sex difference in diagnosis could be explained by differences in symptom severity: boys tended to have more extreme symptoms, and a broader distribution of symptoms, than girls.
“It's an actual neurobiological difference that we're seeing,” says Arnett. It’s not clear why that’s the case, but it could be that girls have a protective effect at the genetic level, she says.
Boys tend to have more severe ADHD symptoms, and more ADHD in general, than girls (Credit: Getty Images)
But the true size of the difference is unclear.
When it comes to real-world diagnoses, boys far outweigh girls. In studies that look at who meets ADHD criteria in the population as a whole, however, the ratio still favours boys, but less so. Depending on which research you look at, the ratio of boys to girls with ADHD could be anywhere between 2:1 and 10:1.
“It would seem to suggest that there's actually a lot more females who are affected by ADHD,” says Florence Mowlem, an associate at healthcare consultancy Aquarius Population Health. “Yet, for some reason that we don’t quite understand, they don't seem to be getting the clinical diagnosis as often as males.”
Research suggests that girls need to have more severe, and more visible, symptoms than boys before their ADHD will be recognised. In one study of 283 children aged between 7 and 12 years old, Mowlem and colleagues looked at what differentiated both boys and girls who met the diagnostic criteria for ADHD from those who had a lot of ADHD symptoms, but not enough to be diagnosed.
Parents seemed to play down girls’ hyperactive and impulsive symptoms, while playing up those of boys
Mowlem, who was PhD candidate at King’s College London at the time, found that parents, in their own ratings, seemed to play down girls’ hyperactive and impulsive symptoms, while playing up those of boys. They also found that girls who did meet the criteria tended to have more emotional or behavioural problems than girls who didn’t. This was not the case for boys.
In a similar study of 19,804 Swedish twins published last year, Mowlem and her colleagues found that girls, but not boys, were more likely to be diagnosed if they suffered from hyperactivity, impulsivity, and behavioural problems.
Girls could also be better at compensating for their ADHD symptoms than boys, similar to how girls with autism mask their symptoms.
Because of social norms, girls with ADHD are less likely to ‘bounce around the classroom’ than boys (Credit: Getty Images)
“Girls are far less likely to bounce around the classroom, fighting with the teachers and their colleagues,” says Helen Read, a consultant psychiatrist and ADHD lead for a large London NHS Trust. “A girl who did that would be so criticised by peers and other people that it is just far harder for girls to behave in that way.”
Even when they are hyperactive, girls are more likely to be over-talkative, or rebellious – a bit of a wild child, she says. That might not be recognised by parents or teachers as being caused by ADHD, especially as we expect girls to be more sociable than boys anyway.But more research is needed before we’ll know how big a problem this is.
If girls are losing out because they have less stereotypical symptoms, they might not be the only ones: boys with purely inattentive ADHD are probably being missed, too.It’s a commonly held belief that girls are more likely to be inattentive than boys. But that’s a myth, says Elizabeth Owens, assistant clinical professor in the department of psychology at the University of California, Berkeley. She says the current best evidence shows that rates of inattention are the same for boys and girls.For a long, long time, ADHD in girls was discounted, or overlooked – Elizabeth Owens
“The inattentive presentation is actually more common [among both boys and girls], but it tends to be under-recognised or under-diagnosed, because the kids aren't typically causing problems in the classroom,” she adds.
In fact, girls and boys with ADHD are much more similar than they are different, says Owens. “It underscores the fact that ADHD and girls is serious. For a long, long time, it was discounted, or overlooked.”Compared to boys with ADHD, girls with ADHD are more likely to develop depression later in life One difference, though, is that girls with combined ADHD – who have both inattentive and hyperactive symptoms – are at higher risk of self-destructive actions as they enter adulthood. Girls with ADHD are also more likely to develop anxiety and depression later in life.
As part of a study that started in the 90s, Owens and her colleagues followed 228 girls, 140 of whom had ADHD, over two decades. At the second and third follow ups, when participants were on average aged 19 and 25 respectively, they found that girls who’d been diagnosed with combined ADHD in childhood were at higher risk of self-harm and attempting suicide.
In theory, recognising and treating ADHD early should help to mitigate this risk – although Owens says that, as yet, there’s no evidence to show this works. “ADHD is a chronic condition,” she says. “It's not something you can treat and it'll go away.”
For adults with ADHD, using a watch to set alerts can be helpful as a reminder to do certain things, such as eat (Credit: Getty Images)
Treatment for ADHD can, however, make a huge difference day-to-day.
Shortly after Johnson-Ferguson was finally diagnosed, she started taking medication, a stimulant commonly used to treat ADHD called lisdexamfetamine. “The next day I just sat down and watched a whole EastEnders,” she says. “It was like walking in slow motion for three days.”
She has to work hard to ensure she reaps the benefits of the drugs – exercising, eating healthily, drinking less, and forgoing caffeine – but the changes have been worth it. “The planning that I can do at work now is incredible, it’s like I’m a different person,” she says.
Many individuals with ADHD take medication to help them with the condition (Credit: Getty Images)
Beyond medication, knowing that the problems you’ve been facing throughout your life are not your fault can also be a huge weight lifted. Johnson-Ferguson describes her life pre-diagnosis as “42 years of feeling completely different to everybody on the planet”.
Now, she’s able to channel the positive aspects of her ADHD – hyper-focusing on short term projects – into a successful career in theatre marketing, while better understanding her shortfalls.
But many are not so lucky. Until we let go of the stereotypical image of what ADHD looks like and get to the bottom of why girls with the condition are being missed, plenty of women will end up living with symptoms that have drastic effects on their lives, without knowing they could get help.
Giving birth can be one of the most painful experiences in a woman’s life, yet the long-term effects that trauma can have on millions of new mothers are still largely ignored.
It’s 03:00. My pillow is soaked with cold sweat, my body tense and shaking after waking from the same nightmare that haunts me every night. I know I’m safe in bed – that’s a fact. My life is no longer at risk, but I can’t stop replaying the terrifying scene that replayed in my head as I slept, so I remain alert, listening for any sound in the dark.This is one of the ways I experience post-traumatic stress disorder (PTSD).
PTSD is an anxiety disorder caused by very stressful, frightening or distressing events, which are often relived through flashbacks and nightmares. The condition, formerly known as “shellshock”, first came to prominence when men returned from the trenches of World War One having witnessed unimaginable horrors. More than 100 years after the guns of that conflict fell silent, PTSD is still predominantly associated with war and as something largely experienced by men.
You might also like these other stories in the Health Gap:
• Why does dementia hit women harder?
• How menstruation changes the brain
• The painful condition that has no cure
But millions of women worldwide develop PTSD not only from fighting on a foreign battlefield – but also from struggling to give birth, as I did. And the symptoms tend to be similar for people no matter the trauma they experienced.
A traumatic delivery can be one of the causes that lead women to develop PTSD after they have given birth (Credit: Getty)
“Women with trauma may feel fear, helplessness or horror about their experience and suffer recurrent, overwhelming memories, flashbacks, thoughts and nightmares about the birth, feel distressed, anxious or panicky when exposed to things which remind them of the event, and avoid anything that reminds them of the trauma, which can include talking about it," says Patrick O’Brien, a maternal mental health expert at University College Hospital and spokesman for the Royal College of Obstetricians and Gynaecologists in the UK.
Despite these potentially debilitating effects, postnatal PTSD was only formally recognised in the 1990s when the American Psychiatry Association changed its description of what constitutes a traumatic event. The association originally considered PTSD to be “something outside the range of usual human experience”, but then changed the definition to include an event where a person “witnessed or confronted serious physical threat or injury to themselves or others and in which the person responded with feelings of fear, helplessness or horror”.
This effectively implied that before this change, childbirth was deemed too common to be highly traumatic – despite the life-changing injuries, and sometimes deaths, women can suffer as they bring children into the world. According to the World Health Organization, 803 women die from complications related to pregnancy and childbirth every day.
Regardless of the statistics, for the women who go through these experiences, there can be a long-lasting impact on their lives
There are few official figures for how many women suffer from postnatal PTSD, and because of the continued lack of recognition of the condition in mothers, it is difficult to say how common the condition really is. Some studies that have attempted to quantify the problem estimate that 4% of births lead to the condition. One study from 2003 found that around a third of mothers who experience a “traumatic delivery”, defined as involving complications, the use of instruments to assist delivery or near death, go on to develop PTSD.
With 130 million babies born around the world every year, that means that a staggering number of women may be trying to cope with the disorder with little or no recognition.
And postnatal PTSD might not only be a problem for mothers. Some research has found evidence that fathers can suffer it too after witnessing their partner go through a traumatic birth.
Regardless of the exact numbers, for those who go through these experiences, there can be a long-lasting impact on their lives. And the symptoms manifest themselves in many different ways.
"I regularly get vivid images of the birth in my head,” says Leonnie Downes, a mother from Lancashire, UK, who developed PTSD after fearing she was going to die when she developed sepsis in labour. “I constantly feel under threat, like I'm in a heightened awareness.”
Lucy Webber, another woman who developed PTSD after giving birth to her son in 2016, says she developed obsessive behaviours and become extremely anxious. “I’m not able to let my baby out of my sight or let anyone touch him,” she says. “I have intrusive thought of bad things happening to all my loved ones.”
Nightmares that cause women to relive the fear, pain and helplessness they felt during childbirth are a common symptom of postnatal PTSD (Credit: Getty)
Not all women who have difficult births will develop postnatal PTSD. According to Elizabeth Ford of Queen Mary University of London and Susan Ayers of the University of Sussex, it has a lot to do with a woman’s perception of what they went through.
"Women who feel lack of control during birth or who have poor care and support are more at risk of developing PTSD,” the researchers write.
The stories from women who have developed PTSD after giving birth seem to reflect this.
Women who feel lack of control during birth or who have poor care and support are more at risk of developing PTSD
Stephanie, whose name has been changed to protect her identity, says she was poorly cared for during labour and midwives displayed a lack of empathy and compassion. A particularly difficult labour saw her being physically held down by staff as her son was delivered. “He was born completely blue and taken away to be resuscitated and I was given no information on his condition for hours.”
Emma Svanberg, a chartered clinical psychologist who is involved in the Make Births Better Campaign, says this is a common theme from the women she hears from.
“The factor which we hear about time and time again is lack of kindness and compassion from staff,” she says.
A study by researcher Jennifer Patterson, at Napier University in Edinburgh, suggests that while midwives are often aware that giving birth can be traumatic for women, they are often so busy they struggle to offer adequate support and information to mothers who may be at risk of PTSD.
Giving busy nursing and midwifery staff more time to care for mothers who have been through a traumatic birth could help to prevent PTSD (Credit: Getty)
Certain groups of women are also more likely to develop postnatal PTSD even before they give birth.
“For women who have a history of prior trauma – perhaps victims of sexual abuse in childhood, those who have previously had PTSD, or depression or anxiety – the risk of developing PTSD is significantly higher. They’re five times more likely,” says Rebecca Moore, a perinatal psychiatrist working for the NHS in East London.
Postnatal processing
The challenge of PTSD resides in the brain. Usually, memories are filed away in the brain’s hippocampus. But if an experience is traumatic, the mind goes into fight-or-flight mode and the part of the brain associated with fear, the amygdala, switches on. This causes memories to become stuck in this primitive part of the brain rather than being safely filed away.
It also means that when something reminds a mother of her experience – such as seeing birth depicted on TV or being in a hospital – the traumatic memories feel less like memories and more like the woman is still in imminent danger, triggering physical reactions like panic attacks or flashbacks.
This broken filing system means “you get a kind of looping of the memory in the mind all the time”, Moore explains.
It may cause structural changes in the brain too. Researchers at the University of California studied the brains of 89 current or former members of the military with PTSD using brain scans to measure the volume of various parts of the brain. It showed that the right amygdala in the brains of military-trained individuals with PTSD were 6% larger than their peers. The right-hand part of the amygdala is particularly associated with controlling fear and aversion to unpleasant stimuli.
“We wonder if amygdala size could be used to screen who is most at risk to develop PTSD symptoms after a mild traumatic brain injury,” says Joel Pieper of University of California, San Diego, who was one of those who led the study.
Millions of women may suffer from postnatal PTSD every year, but stigma surrounding the condition may lead many to try to hide how they are feeling (Credit: Getty)
Whether similar changes occur in the brains of women with postnatal PTSD is not yet known, but it could offer a way of diagnosing those who are affected. The complex mixture of symptoms experienced by women with PTSD after birth can often lead to delays and even misdiagnosis.
Another issue standing in the way of diagnosis is the stigma attached to the condition. Some women feel uncomfortable speaking openly about it for fear of being seen as a failure as a mother, or of seeming ungrateful for their baby.
Svanberg believes birth trauma is a feminist issue. “There is a huge body of research on the disbelief of women's pain, especially marginalised women, and often women's voices are silenced,” she says. Many experts agree that women are simply not listened to or given the information they need to make the best decisions for themselves and their family. (Read more about how women’s pain is more likely to be dismissed than men’s).
“Giving women the facts about different modes of delivery while they are pregnant isn’t scary, it’s empowering,” adds Moore. “Women are capable of making up their own minds, but rarely are they properly informed about risks and treatment when it comes to birth.”
She believes the problem is more of a societal one. “Women are often treated like princesses when they are pregnant, but once the baby is born, it’s all about the baby,” she says. “It’s not uncommon for new mothers suffering with mental illness to hear ‘You’ve got a healthy baby, why are you complaining?’ And it’s then even more difficult for women to pluck up the courage to ask for help.”
It’s thought that half of women with perinatal mental health problems won’t be treated.
“There’s still shame in seeking help and women struggling often fear they will be judged and criticised,” says Moore.
Postnatal PTSD can led sufferers to push away their partner at the time they needed them most (Credit: Getty)
Attempting to keep her condition hidden in this way started to harm Stephanie’s relationships with her husband and her older daughter. Her own PTSD manifested as hyper-vigilance, leaving her in a permanent and exhausting state of being alert and expecting the worst.
“I knew I wasn't OK but kept it hidden for months,” says Stephanie. “I wasn't eating or sleeping. I refused to let anyone look after my son. My other children relied on their dad as I was too focused on my baby.
“My relationship suffered with my daughter, who was just two. I lost all my confidence in my parenting ability when I was always calm and went with the flow before. I pushed my husband and family away.”
Nearly all women involved in the research reported initial feelings of rejection towards their baby
A study led by the University of Sussex confirmed women with postnatal PTSD reported negative effects on their relationship with their partner, including sexual dysfunction, disagreements and blame for the events surrounding the birth. The mother-baby bond was also seriously affected.
Nearly all women involved in the research reported initial feelings of rejection towards their baby and while this changed over time, the study concluded that childbirth-related PTSD can have “severe and lasting” effects on women and their relationships.
For others, it is their career that suffers.
“PTSD has changed my whole life,” says Leonnie Downes, who used to work for the North West Ambulance Service. “I had a good career, and I've had to leave my job to become self-employed just so I can work from home. My wife has had to leave her job too and has become my registered carer. I'm now registered disabled and for the first time ever, we now have to live off disability benefits.”
Some mothers with postnatal PTSD find themselves struggling with exhuasting levels of hyper-vigilance where they feel they cannot leave their baby unattended (Credit: Getty)
Moore says she regularly meets women who are too traumatised to return to work, including paramedics and midwives.
Lucy Webber is one such midwife. “I quit because I couldn't cope with not being able to give women the support they need,” she explains.
But there is help available for women who are struggling with postnatal PTSD, provided they are able to access it. Treatment typically takes the form of medication or cognitive behavioural therapy (CBT) – a talking therapy designed to change the way someone thinks and behaves. Eye movement desensitisation and reprocessing (EMDR) can also be used, which sometimes involves tapping or music to help a patient’s brain remember they are in the present, not trapped in the moment of their flashback. Research also has shown that transcendental meditation can help war veterans with PTSD.
Birth trauma is not that difficult to treat, but it is very difficult for women and partners to access appropriate support – Emma Svanberg
“Birth trauma is not that difficult to treat, but it is very difficult for women and partners to access appropriate support,” Svanberg says, warning that many women are misdiagnosed as having post-natal depression (PND) – another debilitating condition that can follow the birth of a child, but one with a different set of symptoms. In the UK, it can be hard to access treatment in some areas on the NHS, while in other countries, including the US, it can be prohibitively expensive.
But many people believe that mitigation is the answer and that better training for midwives and obstetricians could prevent women developing PTSD in the first place.
Wider acceptance of postnatal PTSD could help to ensure future generations of mothers can enjoy their new baby as a blessing (Credit: Getty)
“The whole system contributes to trauma,” Moore says. “Often women are being cared for by frontline staff, who are doing their job but not with much compassion, because they are burnt out.” The Make Births Better campaign focuses on offering training to medical professionals in an attempt to tackle this. Small changes that cost nothing, such as using kind language and less jargon, can make all the difference in stopping women developing physical and mental problems as a result of giving birth.
Most women would agree that giving birth is a defining and transformative event. And with the right support, good can even come from the most traumatic of births.
Lucy Webber says her experience has helped her become a gentler parent and Stephanie has even decided to become a midwife.
Almost two years on, my own life is gradually getting easier, but I approach my daughter’s birthday with a mixture of excitement and trepidation because of the memories and physical reactions it will undoubtedly trigger. She is the best gift I could ever hope for and her birthday will also be a celebration of how far we have come since her arrival.
Besides the little toy guitar we will be giving her, perhaps the best gift I can offer is to play my own small part in challenging the norms of what it is to give birth and be a mother, so birth trauma and postnatal PTSD can be dealt with in the open.
How we’re tackling gender imbalance
An estimated 10% of women have this condition, which can include debilitating pain. But it’s underresearched, poorly understood – and still without a cure.
By Aimée Grant Cumberbatch
My painful periods started when I was about 14. I wore heat patches to school in the hope that they would help me last through the day. Sometimes they did. But sometimes I ended up in sick bay writhing in agony on the fold-out bed, where the receptionists didn’t know what to suggest because I’d already had my appendix removed.Ten years of pain later, I’m finally in the process of being diagnosed with endometriosis. But far from simplifying my issues, what I’ve seen during my many doctor’s appointments is that the disease remains poorly understood – and that its diagnosis and treatment can be a complicated and life-long ordeal.
Endometriosis is a gynaecological condition associated with menstruation where tissue similar to the lining of the womb is found in other areas of the body, including the fallopian tubes, pelvis, bowel, vagina and intestines. In rare cases it has even been found in the lungs, eyes, spine and brain – in fact, the only place in the body it has never been found is the spleen. Symptoms include severe, sometimes debilitating, pelvic pain, fatigue and heavy periods.
Endometriosis is estimated to affect one in 10 women of reproductive age While there are many lesser-known health conditions which are underfunded and under-researched, few are as common as endometriosis, which affects about 176m people globally. In the US, where, as in other countries, it’s estimated to affect one in 10 women of reproductive age, it receives about $6m (£4.7m) in research funding each year. Sleep research alone receives more than 50 times that amount.
Pain isn’t the only consequence of endometriosis. One study across 10 countries found that endometriosis costs each patient an average annual total of €9,579 (£8,600) in healthcare, productivity and quality of life costs – that’s more than €26 (£23.45) a day. It may be linked to infertility. And then there is the chance that the pain itself makes patients vulnerable to other conditions.
“We have good evidence that having serious pain alters your central nervous system, alters how you respond to pain in the future and makes you potentially more susceptible to other chronic pain conditions,” says Katy Vincent, a senior pain fellow at the University of Oxford.
The primary symptom is usually acute pelvic pain with no obvious physical cause (Credit: Alamy)
For women who are symptomatic, and many are not, the primary symptom is usually acute pelvic pain with no obvious physical cause. That may make it enigmatic. But that it was a health condition experienced only by women – and is linked to menstruation, in particular – has made it more of an enigma than it perhaps could be.
Ancient origins
Microscopic discovery of endometriosis is most often attributed to Czech scientist Karl von Rokitansky in 1860, though this is disputed and previous more rudimentary microscopic discoveries have also been recorded. Records of endometriosis-like symptoms, meanwhile, date back to antiquity. It also has an overlap with the condition ‘hysteria’, which derives for a Latin word for “of the womb”: one study of representations of pelvic pain in medical literature found that many cases dismissed as “hysteria” may well have been endometriosis. “The original meaning of hysteric convulsions during this era generally referred to women falling to the ground, doubled over in a foetal position,” the study notes. “They could very easily be describing a response to acute abdominal pain.”
Many cases dismissed as ‘hysteria’, in which symptoms included convulsions from pain, may well have been endometriosis (Credit: BBC/Getty)
The historic underestimation and misunderstanding of endometriosis continues to inform modern medicine. Researched less than other conditions, it’s also less understood. The cause of endometriosis is not known. There is no cure. It often takes up to around a decade to get diagnosed, and the only means of definitive diagnosis is a form of keyhole surgery known as laparoscopy.
I never remember a single GP or hospital doctor, anybody, saying the word ‘endometriosis’. Or just even asking the right questions – Alice Bodenham
I spoke to three women now diagnosed with endometriosis, all in their 20s and 30s. Along the way, all three had been misdiagnosed with other conditions and had their symptoms dismissed or underestimated. “I never remember a single GP or hospital doctor, anybody, saying the word ‘endometriosis’. Or just even asking the right questions,” says Alice Bodenham, 31. “It’s very much ‘it could be this’, or ‘you’re making it up’.”
Part of the problem is the systemic tendency to dismiss women’s pain, when pain is of the most common symptoms of endometriosis. I experienced this myself when I found one internal ultrasound scan acutely painful and informed the doctors: I later received my results in the post with the note “patient experienced mild discomfort during scan”. Making matters worse, there’s no correlation between the level of pain experienced and the severity of an individual’s condition.
Women often find their pain symptoms being dismissed (Credit: BBC/Alamy)
As there are no non-invasive means of definitive diagnosis, without a physician believing a patient’s description of symptoms, there’s no referral for a diagnosis. But women’s symptoms, too, are often dismissed as being “all in your head”.
One UK survey found of 2,600 women with endometriosis found that 40% had visited the doctor 10 or more times before being referred to a specialist
It may be little surprise, then, that one UK government survey of 2,600 women with endometriosis found that 40% had visited the doctor 10 or more times before being referred to a specialist. Bodenham, for example, collapsed multiple times before her pain was taken seriously.
Caitlin Conyers, 24, who runs the blog My Endometriosis Diary, began to suspect she might have the condition through her own research, but this was dismissed by her physicians. “About three years ago I ended up in an urgent care centre. I’d been Googling the different causes and one was endometriosis and I did suggest this to the doctor at the time and they just said, ‘Oh no, it definitely isn’t that’,” she says. “I explained that I had really bad period pain and general abdomen pain and they still said no.”
Oxford’s Vincent isn’t hesitant about whether gender plays a role. “If every 14-year-old boy went to the GP saying, ‘I miss two days of school every month’, they would stop missing school every month,” she says.
Physicians sometimes fail to find evidence of lesions on initial scans (Credit: BBC/Alamy)
Making matters more complicated, physicians also sometimes fail to find evidence of lesions on initial scans, particularly if the lesions are superficial. Endometriosis forums are littered with stories of false negative ultrasound scans.
A lack of awareness on the patient side can delay diagnosis too. Menstrual taboos still persist and two of the women I spoke to reported being told, whether by family or through sexual education, that periods might be painful or uncomfortable. What they never understood was how painful (or not) a normal period should be.
Menstruation taboos mean that many women don’t know how painful (or not) a normal period should be (Credit: BBC/Alamy)
Endometriosis charities and campaigners around the world are working to raise awareness, and their efforts seem to hav helped. In 2017 the Australian government launched a National Action Plan For Endometriosis which seeks to “improve the treatment, understanding and awareness” of the condition, and increased funding to A$4.5m (£2.5m), new clinical guidelines and – crucially – for the subject to be made part of primary healthcare professionals’ medical education. In the UK, government advisory body the National Institute for Health And Care Excellent (Nice) released guidelines in 2017 with the aim of standardising diagnosis and treatment pathways for patients.
But while that’s a good step in the right direction, there already are many guidelines for GPs to juggle, says Anne Connolly, clinical champion for women’s health at the Royal College of GPs. Lone Hummelshoj, chief executive of the World Endometriosis Society, adds that the lack of specialist centres is another worldwide problem.
No quick fix
Even after a diagnosis is reached, symptom management is by no means straightforward –and misinformation persists here too.
Some medical practitioners still tell patients pregnancy is an effective treatment (Credit: BBC/Alamy)
Some medical practitioners still tell patients pregnancy is an effective treatment. One physician this year told me she suspected endometriosis – but, she added, “there’s not much we can do unless you fancy getting pregnant”. Given that the disease can impact fertility of patients, this seems at the very least insensitive. It’s also inaccurate: while it may relieve symptoms of endometriosis, it’s only for the duration of the pregnancy.
Meanwhile, writer and performer Lena Dunham raised the profile of hysterectomy as a treatment for endometriosis by writing about her choice to undergo the surgery in Vogue US earlier this year. But its use as a treatment for endometriosis is controversial. As the condition is characterised by lesions outside of the uterus not inside of it, its removal is by no means a cure and endometriosis can recur afterwards.
Hysterectomy is by no means a cure and endometriosis can recur afterwards
Because the development of endometriosis lesions is controlled by oestrogen, hormonal treatments are often one of the first prescribed. These can help manage the condition, but do not cure it, and can have their own side effects. A 2016 study by researchers in Denmark found that women using hormonal contraceptives were more likely to seek treatment for depression. (Watch our video on eight women who experienced serious side effects from the contraceptive pill).
Hysterectomy is not a cure, and endometriosis can occur afterwards (Credit: BBC/Getty)
Another potential treatment is medical menopause. However, it is not a long-term option because it can affect bone density, particularly in young people, and, although rare, one of the potential side effects cited by the brand Zoladex is accidental full menopause. Cook told me there is a lack of informed consent around the use of this treatment. She says, “One of the things I hear a lot of is the number of women who end up taking drugs or having injections to go into medical menopause and they do not realise that’s what it is.”
As such, there is research ongoing into potential alternatives.
“Drug treatments for endometriosis are entirely focused on hormones and we need something else because we know for a lot of women that doesn’t work very well,” says Krina Zondervan, a professor of reproductive and genomic epidemiology at the University of Oxford. “And it gives a lot of side effects that women are not that happy to experience in the long term.”
Although they treat only the symptoms, not the condition, painkillers are another option. But they aren’t without adverse effect, either. Bodenham tells me how the opioid painkillers she’s been taking for the past three years have left her with a constellation of side-effects including “anaemia and hypertension”. She says, “I used to run a 5k every week… and now some days just walking downstairs to get a glass of water feels like doing a marathon.”
While painkillers can help with endometriosis symptoms, their side effects can be major (Credit: BBC/Alamy)
Despite this, Bodenham feels lucky to receive them – she knows trying to access strong painkillers can lead to accusations of addiction. (There is also a risk that use of opioid painkillers will lead to abuse or dependency, although this is small among those with no history of substance abuse or addiction.)
There is some hope. The illness’ profile is on the rise and efforts are being made to educate GPs and patients about pelvic pain. But as patients wait for the medical system to catch up, their symptoms are still being misunderstood and their illnesses misdiagnosed with serious mental and physical health consequences.
Having found that birth control adversely affected my mental health, my next step is deciding whether to start treatment via the Mirena coil’s low dose of hormone, or to continue pursuing a definitive diagnosis via laparoscopy. But laparoscopy would require several weeks of recovery – and as a freelance writer with little job stability, I would need more savings than I have. It’s one more example of the difficult choices women with chronic pelvic pain face every day.
Correction: A previous version of this story inaccurately described one of Krystal Rodriguez’s symptoms as collapsing. This has been changed. We regret the error.
How the pill changes your body shape
Many women believe that the pill can cause weight gain. Research hasn’t found this – but it has found that it can change body shape (and fat storage) in other surprising ways.
By Zaria Gorvett
It’s been blamed for polluting our rivers, destroying our marriages and – ironically – killing our sex drives. It’s been called a conspiracy by the patriarchy. It’s even be accused of making women fancy ugly men. But for many women, one of the most off-putting charges against the contraceptive pill is that it makes us fat.In fact, weight gain is the most commonly reported side effect of the combined pill – the most popular type, which contains both lab-made oestrogen and progesterone. This is why pharmaceutical companies list it on the packet.
But after several decades of research, there still isn’t any conclusive evidence that the effect is real. The largest review so far examined 49 studies of the combined pill and found “no large effect is evident”, but also that there wasn’t enough well-conducted research to be sure. The researchers found this is true no matter what type of progesterone the combined pill contained (for more on the different kinds of pill, check out this article). Other studies that looked at progesterone-only pills similarly have found little evidence of an effect.
Maria Gallo, an endocrinologist at Ohio State University who co-authored the review, believes our belief in the pill-weight connection is down to a natural human bias. People are experts at finding patterns all around us, even where there are none. The phenomenon, known as apophenia, is the reason we may find it easy to compare peppers to politicians, see the faces of Harry Potter villains staring down at us from the clouds, or read too much into past lottery numbers. We’re particularly susceptible to apophenia if we’ve been primed to expect a certain outcome – such as gaining weight after starting a new medication.
“It’s the same reason why there’s this idea that vaccines can cause health problems,” says Maria Gallo. “If you give them to a population, you’re going to have some people who have health problems, whether they’re linked to the vaccine or not.”
Researchers haven’t found evidence that the pill causes weight gain – but they have found that it can change a woman’s body shape and body fat percentage (Credit: Getty/BBC)
In the case of the pill, Gallo points out that the average person puts on just over a pound (half a kilo) of weight each year for most of their life, starting in early adulthood – which, incidentally, is when most women start using contraception. It may be reassuring to be able to blame this ‘weight creep’ on something other than overeating; last year she even caught women in the act of inventing weight gain after being fitted with the contraceptive implant.
Even so, it’s not all in our heads. Though large-scale reviews haven’t found that the pill causes weight gain, it can change a woman’s body shape and composition.
There are three big reasons for this, and they have to do with muscle, fluid retention, and fat.
Muscle in
Back in 2009, Steven Riechman, an exercise physiologist at Texas A&M University, discovered one surprising impact of the pill, entirely by accident.
Women on the pill had gained 40% less muscle than those who weren’t on it
At the time, he was researching how a person’s genetic makeup can affect their ability to grow their muscles through exercise. His research team put a group of men and women through 10 weeks of resistance training – slow, punishing exercises such as crunches and lifting heavy weights. Then participants were weighed to see if they had more muscle than they started with. The team also gathered information on various lifestyle factors so that they could make sure any gains were caused by genetics and not, for example, the medications they were on.
While they were doing this analysis, they discovered that women on the pill had gained 40% less muscle than those who weren’t on it.
“It jumped out as a pretty big impact,” says Riechman.
Eight women open up about the side effects they experienced from the pill. Watch the video below.
It’s well-known that men naturally have more muscle than women. The average man has 72lbs (33kg) of brawn, compared with a measly 46lbs (21kg) in women. This is partly just because men are taller and heavier overall, but that isn’t the whole story – as a percentage of overall body mass, men are about 38% muscle while women are 31%. This comes down to hormones: men have more ‘anabolic’ hormones running through their veins, which tell the body when to grow more muscle.
Men tend to have a higher percentage of muscle mass than women because of their hormones (Credit: BBC/Getty)
This includes an important but little-known steroid called DHEA. It’s secreted by the adrenal glands – cocktail sausage-sized organs which sit above each kidney – and is involved in everything from keeping bones strong to maintaining our immune systems.
The hormone used to be extremely popular with athletes, partly because of its extraordinary muscle-building power, and partly because doping with it was legal until fairly recently. Just in case you were getting any ideas, it also has many drawbacks, such as the tendency to cause liver damage and shrink a man’s testicles.
But women produce anabolic hormones too – and the team found that those on the pill had much lower levels of DHEA in their blood.
When they worked out, women on a certain type of pill had less of the muscle-building hormone DHEA – and less muscle gain – than those not on the pill (Credit: BBC/Getty)
Even more intriguingly, the poor muscle gains weren’t found in all women on the pill, just those that contained a certain type of lab-made progesterone that likes to bind to the same protein.
“We’re pretty confident the progesterone is what’s causing this,” says Riechman. One possibility is that by competing for the same binding sites, the hormone may be blocking signals to grow more muscle. The results haven’t definitively proven the link, but if it does turn out to be real, surely women will want to know about it – especially in the light of recent fitness obsessions such as CrossFit and Instagramming your abs. “This study should absolutely be followed up. People are interested and we get calls fairly regularly about it,” he says.
Fat storage
And the pill may be changing women’s bodies in other ways, too. Just as it has an impact on the proportion of muscle in our bodies, it could be exerting subtle influences on fat – particularly where it is stored in the body.
The pill could be exerting subtle influences on fat – particularly where it is stored in the body
At puberty, oestrogen and progesterone are responsible for the development of typically ‘female’ characteristics, such as wider hips and larger breasts, largely by changing the way fat is distributed. The hormones are also often given to transsexuals for the same reason.
The womanly ‘hourglass figure’ emerges as different kinds of fat tissue respond differently to these reproductive hormones. For example, subcutaneous fat – the kind of chub that women carry around their thighs, hips and breasts – contains lots of oestrogen receptors.
Because hormones react differently with each type of fat tissue, changing a woman’s hormone balance could alter where her fat is stored (Credit: BBC/Getty)
It’s easy to see how, theoretically, changing a woman’s hormone balance could alter where her fat is stored. Some research has borne this out: one early study found that women on pills with higher levels of oestrogen tended to have pear-shaped bodies and more subcutaneous fat, though not necessarily more fat overall.
Cell swell
Finally, there’s the top menace of many women on the pill: bloating.
That icky, swollen feeling happens because oestrogen also affects the way the body metabolises water, by influencing the production of certain proteins in the kidneys. The end result is that the body retains more fluid than it usually would. This then seeps into fat cells, causing them to swell up. Because women tend to store more fat in their breasts, hips and thighs, these areas can expand the most.
Oestrogen can cause the body to retain more fluid, including the type used in the contraceptive pill (Credit: BBC/Getty)
Synthetic oestrogen is six to 10 times more potent than the natural kind
This also happens on a smaller scale in women who aren’t on the pill, during the week just before their period. But it’s exaggerated by the contraceptive because synthetic oestrogen is six to 10 times more potent than the natural kind, and because it’s taken nearly every day, which means the levels of both hormones are more constant.
So while the pill may not be leading to long-term weight gain, some women could still find that their clothes fit differently.
Fluid retention may also help to explain why some women report that the pill increases their cup size. There have been very few studies into the effect – understandably, most research tends to focus on breast cancer rather than size – but back in the 1990s a couple of Swedish scientists decided to take a look.
The contraceptive pill is known to increase a woman’s risk of developing breast cancer slightly, both while she’s taking it and in the 10 years afterwards. The researchers wanted to know whether this might be because these women have larger breasts; there’s an inherent risk in having (or growing) more cells, which is one reason tall people tend to be more susceptible to cancer.
To find out, the team tracked the monthly cycles of 65 healthy women who either were on the pill, used to take it, or had never taken it. They found that not only did pill users have significantly larger breasts overall, but they were especially large at certain times of the month. Women who had previously been on the pill had an average-sized bust.
One study found that the pill appears to increase breast size, and not just from water retention (Credit: BBC/Getty)
The team didn’t check the women’s chest measurements before they started taking the pill, so it could be argued that these women had always had larger breasts. However, it seems likely this was due to the contraceptive pill, because their breast sizes weren’t linked to the normal factors you’d expect – such as their height, BMI, or body weight – as in the women who weren’t on the pill.
The hormones in the pill are actually causing women’s breasts to grow
Exactly how this happens remains a mystery. The breast expansion could just be swelling from fluid retention, but another possibility is that the hormones in the pill are actually causing women’s breasts to grow. For example, the burst of growth that happens each month, and is necessary to maintain a constant size, could be lasting a bit longer. This would lead to more tissue overall – and explain the heightened cancer risk.
Of course, whatever subtle effects the pill has on your figure – for better or for worse – millions of women feel that it’s worth it. As one Reddit user put it, no birth control at all is likely to lead to 25 to 35 pounds (11-15kg) of weight gain over the course of nine months.
Why children become bullies
In India, women have died getting sterilised – but it remains the most popular contraceptive method both there, and overall worldwide. Why is it so popular? And what are the drawbacks?
Author image
By Hannah Harris Green
11th September 2018
Raji Kevat of Ganiyari, Chhattisgarh, has mixed feelings about tubal ligation, the most common form of female sterilisation. It is an operation that she has undergone herself. After she received the procedure in 2014 at one of the Indian government’s now-infamous sterilisation ‘camps’, she advised her sister-in-law, Shiv Kumari Kevat, to do the same.
Shiv Kumari and 82 other women lined up in an otherwise abandoned hospital in the city of Bilaspur in November 2014. The surgeon cut the women with a single instrument, allegedly without changing his gloves between each surgery. The women were then laid on the hospital floor to recover.
That night, Shiv Kumari began vomiting and experiencing terrible pain in her gut. She was dead within days. While the government’s official explanation was that the deaths happened due to compromised drugs, a post-mortem report showed that Shiv Kumari had passed away due to septicaemia – likely from surgical infection. She was one of 13 women who died from the camp.
One of the women who suffered complications during the 2014 mass sterilisation that killed 13 women, Anita Bai tends to her child while under care in hospital (Credit: Getty)
Still, says Raji, if anyone asked her, she would advise them to get the procedure, even after losing a family member. Her reason is simple.
“If you don’t, your family will get too big,” she says.
Like many women around the world, Raji considers sterilisation the only real contraceptive option.
You might also like these other stories in the Health Gap:
• The strange truth about the pill
• The birth control women don’t know
• The dark side of the pill
An average of 19% of married or in-union women rely female sterilisation globally
If you look at the world as a whole, female sterilisation is the most popular form of contraception. While the pill tends to be more common in Western Europe, Canada or Australia, for example, sterilisation is often the main choice for women elsewhere, including much of Asia and Latin America. According to a 2015 UN survey, the most recent available, an average of 19% of married or in-union women relied on female sterilisation globally – the next most popular method, the IUD, is less than 14%, while the pill is just 9%.
And sterilisation is more popular in India than it is anywhere else. In India, the figure for female sterilisation is 39%, almost twice as much as the worldwide number.
Sterilised history
Government sterilisation programmes began in the United States. In 1907, the state of Indiana passed a law requiring institutionalised persons to be sterilised – the world’s first eugenics law.
The world’s first eugenics law was passed in Indiana in 1907, when the state required that institutionalised people be sterilised (Credit: Wellcome Collection)
Nazis would later use California’s racist eugenics programme as precedent for sterilising Jewish people
Many other US states passed similar laws. Nazis would later use California’s racist eugenics programme as precedent for sterilising Jewish people. Eugenics laws in the US would mostly be overturned by the 1970s, but they overlapped with the rise of the pill, feminism and the sexual revolution. And it was during this time that governments of recently colonised countries, including the Philippines and Bangladesh as well as India, would also begin to sterilise their populations, with international support. Peru and China also received foreign aid for their sterilisation programmes.
But today, India is the country where the most sterilisations are performed in the world, in terms of both absolute numbers and percentage of the population.
These high numbers might be partially explained by India’s history as the world’s first country to have a department devoted to family planning, which emphasised sterilisation early on. The Indian government began aggressively promoting sterilisation in the 1970s, and a number of international organisations and governments were happy to provide support, including the World Bank, the US government and the Ford Foundation.
A cancelled stamp promotes support for India’s family planning policies (Credit: Getty)
In a 1977 interview with the St Louis Dispatch, RT Ravenholt, director of the US Office of Population, said that the government’s goal was to sterilise a quarter of the world’s fertile women – around 100 million. His argument was that since US medical advances were responsible for the expansion of the world’s population, they should also be responsible for keeping it down… albeit through women’s bodies, rather than men’s.
Today, USAID, the arm of the US government that provides funding for family planning services around the world, continues to support some of this thinking: a USAID-funded white paper in 2014 recommended that sterilisation increase globally.
After a forcible male sterilisation campaign when more than six million low-income men were sterilised and 2,000 died, the Indian government began to change its official approach to family planning.
Indian officials moved away from setting ‘targets’ for the number of people who ought to be sterilised and began investing more in reversible methods of contraception, like the pill. Over the last two years the Indian government rolled out Mission Parivar Vikas, which offers three new hormonal methods of contraception, including progestin-only contraceptive pills.
Sterilisation isn’t only popular in India – it’s on the rise
Even so, sterilisation isn’t only popular in India – it’s on the rise. According to UN Statistics, globally the proportion of married or in-union women who have been sterilised has decreased from 20.5% to 19% over a decade – but in India it has risen from 34% to 39%. Government sterilisation camps, meanwhile, continued until 2016.
Doctors prepare for a sterilisation procedure at Delhi’s Sucheta Kriplani Hospital (Credit: Shahid Tantray)
The irreversibility of sterilisation also means that one cannot fairly compare its popularity with that of other methods. Most studies, including the UN survey, count how many women are currently using a type of contraception. While women can, and do, choose to discontinue other methods at any time, once their contraceptive method is sterilisation, that rarely changes: tubal ligation reversal is both costly and likely to fail.
Still, that makes the difference between the numbers of sterilised women globally, versus in India, all the more marked.
Permanent fix
For women around the world who know they don’t want children or for mothers who have reached their desired number of children, sterilisation is often a safe and effective option. In the US, for example, many new mothers opt for sterilisation right after childbirth, and other women will switch from spacing methods (like condoms or the pill) to sterilisation once they’ve completed their family.
The upside is that these women never have to think about contraceptive methods again. They’re also unlikely to have side effects once they’ve recovered from the procedure.
But sometimes, as in Chhattisgarh, women received the sterilisation procedure without fully understanding its significance – and in unsafe conditions. What happened in Bilaspur “was a tragedy waiting to happen”, says Yogesh Jain, director of Jan Swasthya Sahyog hospital in Ganiyari, near Shiv Kumari’s home. He considers the deaths an inevitable result of policy choices that devalue poor women. “I could have written about this 10 years ago that something's going to happen,” he says, adding that the women were treated as no more valuable than “a uterus and a pair of hands”.
Roop Chand Srivastava holds an image of his wife Phool Bai, who died during the November 2014 mass sterilisation in Bilaspur (Credit: Getty)
In an investigation of the sterilisation camp deaths in Chhattisgarh, the Population Foundation of India (PFI) found that the state government spent about 20 times the amount incentivising women to get the procedure as they spent on the procedure itself – and women were only paid between 600 and 1400 rupees each (£7-15) to get sterilised. But because of the 2014 tragedy, the national government “did wake up to the fact that there is abysmal quality of care in these facilities”, says PFI director of programmes Sonal Sharma. She says the Indian government accepted PFI’s recommendation that the ‘camp’ approach to sterilisation be banned.
The government has shifted the focus instead to ‘fixed day’ services, meaning that women must come to particular facilities on particular days of the week if they want to be sterilised – which allows better monitoring and regulation of operating room conditions. But in some places, the more limited hours are proving inadequate to service demand for the procedure. At the Mungeli district level hospital about 50km from Bilaspur, for example, a surgeon now comes in to do the procedure two days each week. But that only adds up to about 20 surgeries – which, says the district’s chief medical officer Mukhya Chikitsa, isn’t enough for all the women who want it.
If sterilisation remains in such high demand even among women in Chhattisgarh despite its now-tainted history there, many women must still see it as their best option.
But the procedure remains controversial – and not only because of preventable deaths like those in Bilaspur.
Imperfect answer
Even when performed correctly and in hygienic circumstances, tubal ligation remains more risky and invasive than vasectomy. Even so, in the majority of countries, female sterilisation is more popular than male sterilisation.
Even when performed in hygienic conditions, tubal ligation remains riskier than vasectomy – but in India and other countries is the far more common choice (Credit: Shahid Tantray)
The nature of tubal ligation also gives rise to ethical concerns: compared with other types of contraceptives, it is easier to implement without a woman’s full consent or understanding. A woman must follow instructions to use methods like the condom or the pill. But once a woman is sterilised, her participation in controlling her fertility is over. Governments have abused this. In Peru in the late 1990s, for example, public medics would sterilise poor women without telling them, instead claiming to be performing a different procedure like injecting vitamins intravenously.
Most women who get sterilised in India never use another contraceptive method first to help space out pregnancies, which comes with significant health risks
One other difficulty is that the emphasis on, and popularity of, sterilisation can encourage women not to use other methods. Most women who get sterilised in India use only this contraceptive method in their lifetime. In other words, they never use something like an intrauterine device (IUD), patch or pill first to help space out pregnancies. This comes with significant health risks: not spacing out pregnancies means that both the women and their children face an increased risk of death and other complications.
This goes hand in hand with the fact that other contraceptive methods, like the pill or IUD, are less available in the country, as are trained professionals who can insert IUDs. And across social classes, women tend to lack knowledge about other methods.
Most women who get sterilised in India have never previously used another contraceptive method (Credit: Shahid Tantray)
Madhu Goel is a gynaecologist at Fortis La Femme, a high-end private hospital for women in Delhi’s Greater Kailash neighbourhood. Even among her patients, sterilisation is still “the method” of contraception, she says. Though that’s especially true of older women, younger patients also have misgivings about alternatives. Even most young women who spoke with her after researching contraception on the internet had misconceptions about the pill – believing that it causes permanent infertility, for example.
But Goel says that, at least among her patients, social change in India means that more women are educating themselves about other options. Divorce rates in India are going up, for example. As a result more women want to reverse their sterilisations, hoping to start new families with their second husbands.
Policy may eventually have an effect, too. The National Policy for Women laid out by the ministry of Women and Child Development in 2016 outlines a shift focus from female to male sterilisation. But according to experts, this policy has yet to be put into practice.
Given the international machine that has made female sterilisation so popular in India, it might take time to make a real dent in its dominance.
This story was reported with support by the Pulitzer Center for Crisis Reporting.
6th September 2018
What closely resembles an alien insect and decapitates sperm? If you answered the ‘coil’, otherwise known as the intrauterine device (IUD), congratulations! You’re correct.
About the length of a paperclip, these bizarre objects come in a wide range of shapes, from frilly ovals to four-legged spiders. However, the most common variety in the Western world consists of a T-shaped piece of plastic with a dangling ‘tail’ of threads.
To work, IUDs must be placed inside the womb, where they can remain – depending on the brand and type – for up to 12 years. They’re incredibly good at preventing pregnancy.
In Asia, 27% of women use an IUD for contraception; in North America, 6.1%
In fact, they’re the most effective contraception on the planet – aside from sterilisation or avoiding sex altogether. And apart from those options, they’re also the most popular birth control method worldwide. But that doesn’t mean that most women in every country have heard of them. In Asia, for example, 27% of women use an IUD for contraception. But the rate is just 6.1% in North America… and less than 2% in Australia and New Zealand.
Why is this? And why should more of us know about them?
You might also like these other stories in the Health Gap:
• The strange truth about the pill
• How the menstrual cycle changes women’s brains
• The excruciating condition that only affects women
One reason IUDs aren’t more widely used in the United States might be the lack of marketing. Over the years, pharmaceutical giants have chosen to invest heavily in promoting the contraceptive pill instead, which is more profitable.
“I think patients now are more aware than they were in the past,” says Alyssa Dweck, a gynaecologist based in New York. “But money is obviously important.”
Today’s IUDs are tiny, T-shaped devices no bigger than 32mm by 36mm (Credit: BBC/Getty)
“There are many companies, with many different formulations [of contraceptive pill], with some of the differences hardly noticeable to individuals,” says David Hubacher, an epidemiologist at the non-profit human development organisation FHI 360. “In contrast, if you look at the main IUD we’ve had on the market since 1988, ParaGard, there hasn’t been much advertising.”
Another reason is that they have a bit of an image problem. There are plenty of hostile rumours about IUDs out there – like the idea that they’re painful, cause infertility, or lead to bad sex. In the light of their checkered history, this isn’t particularly surprising.
The idea that placing a foreign object in a woman’s reproductive organs could prevent pregnancy first emerged in the late 19th Century. To begin with, doctors were pretty much just placing random objects in the cervix, the entrance of the uterus, and hoping that this would do the trick. These early precursors to the IUD, called “stem pessaries”, were made from all kinds of materials, such as bone and cat guts. But later versions were mostly metal screws with long, forked ‘tails’.
Past physicians experimented with contraceptives like this ‘wishbone pessary’, developed in Germany around 1880 (Credit: BBC/Science Museum, London)
The first mainstream IUDs emerged several decades later, in the 1920s. These were popularised by a German doctor Ernst Grafenberg, who is better known today for having the ‘G spot’ named after him.
Grafenberg’s design was a simple ring of metal that was placed in the womb, and he soon began performing scientific studies to see if they actually worked. All was going well, but their development was cut short when the Nazis arrested him. He was later rescued by the queen of birth control, Margaret Sanger, and fled to the United States.
Ernst Grafenberg designed this IUD in the 1920s (Credit: BBC/Science Museum, London)
From then onwards, IUDs really took off. In China, IUDs were an important tool for implementing the one-child policy, along with forced sterilisations. To this day, the country has its own devices which have been especially designed or altered to make them more difficult to remove; they often require surgery.
In America, meanwhile, there was the Dalkon Shield disaster. This infamous brand, which had a broad ‘shell’ a bit like a horseshoe crab's, was introduced in the 1960s. They were based on the idea that IUDs with a larger surface area would be more effective. Instead, they had an unacceptably high risk of pregnancy. Even worse, they also led to widespread infections and infertility. It was a massive public scandal and more than 50,000 women ultimately filed successful lawsuits against the manufacturer.
“Women are always going to be concerned about their future fertility. It took a long time to make IUDs in a way that was considered safer, and to reorient women’s views,” says Dweck.
Introduced in the 1960s, the Dalkon Shield had a high risk of pregnancy – and of infections (Credit: BBC/Science Museum, London)
Luckily, modern versions are quite different. There are two main types: those that contain copper, and those that slowly release a low dose of the hormone levonorgestrel.
“The products we have today are very safe and effective,” says Hubacher. He points out that even when IUD use was at an all-time low, IUDs were five times more popular with female doctors than the general public. “And if you just look at the subset who were OB-GYN [specialists in reproductive medicine], the rates were up to nine times higher.”
To get to grips with this enthusiasm, it helps to compare them to other contraceptives.
If you take the pill the human way, over 10 years you have a 61% chance of getting pregnant
Millions of women across the globe, from Melbourne to Mumbai, woke up this morning and punched a small pill out of its packet. They must remember to take one nearly every day, which is surprisingly difficult.
Theoretically, the combined contraceptive pill gives women less than a 1% chance of becoming pregnant in any given year. In reality, most of us accidentally miss around five pills each month – so the rate of pregnancy is actually more like 9%. That means that if you take the pill the human way for 10 years, you have a 61% chance of getting pregnant overall. In other words, more likely than not, you will get pregnant. (Find out more about the pill in our recent stories on eight women's stories of side effects and the 'masculinising' effect it can have on women's brains).
Millions of women rely on the contraceptive pill, but not all realise that there is a 61% chance of becoming pregnant on it over a decade (Credit: Getty Images)
By one estimate, reliance on oral contraceptives leads to 960,000 pregnancies every year. There are also side effects, such as an increased risk of potentially life-changing blood clots and a faded sense of wellbeing.
The issue of compliance is common to most contraception, from condoms to the contraceptive patch. Human nature (and sexual behaviour) being what it is, these just aren’t used in real life as they are intended.
But IUDs are different. Because they require no maintenance aside from insertion, which is done by a medical professional, they’re exactly as effective as they say on the packet. Copper IUDs give women roughly a 1% chance of getting pregnant each year, which works out as an 8% risk over 10 years; hormonal versions provide less than a 1% chance each year or a 2% chance over a decade. The hormonal version comes with what many women see as an added bonus – one in five users find that their periods stop altogether.
Anna Foley, from New Zealand, decided to get a hormonal IUD a few years ago. “In general for me, I loved it because I always sucked at remembering to take the pill,” she says. “Plus I found that I had some negative side effects to the hormones, while the Mirena [IUD] had a lower dose.”
People used to think that IUDs mainly worked after conception, by making it impossible for a fertilised egg to implant. But experts no longer believe this to be the case.
Instead, IUDs work for two reasons. The first is that any object in the womb leads to an inflammatory response: a certain type of white blood cells rushes to the area, where they eat sperm and produce waste that is toxic to sperm. One study found that IUDs increased the number of these cells in the womb by 1,000%.
The IUD has come a long way since this version, made of catgut loop and bone, used in the early 20th Century (Credit: BBC/Science Museum, London)
The second reason depends on the type of IUD. Hormonal versions modify a woman’s body to make it more difficult for sperm to reach a woman’s egg, and make her womb inhospitable in case one is fertilised. Copper IUDS, on the other hand, are fearsome sperm killers. As copper ions dissolve into the womb, they paralyse and even decapitate sperm – though exactly how remains a mystery.
Still, even modern IUDs come with some risks. The most serious is the possibility the device will be pushed through the wall of the uterus while it’s being inserted, which is classed as a medical emergency but only happens very rarely (one in every 1,000 insertions). There is also a slight increase in the risk of infections, pelvic inflammatory disease and of ectopic pregnancy among other things, but these disappear once it is removed. Of course, other methods of contraception come with risks too – roughly one in every 1,176 women on the pill are at risk of developing a blood clot in any given year, for example.
In terms of the intensity of the pain, I would have told you it was a 10/10 – Anna Foley
But one major concern many women have is that having an IUD inserted will be painful. And while this isn’t always the case, it certainly can be. Foley doesn’t mince words about her own experience. “In terms of the intensity of the pain, I would have told you it was a 10/10. It was really, really bad. And whenever I thought about the pain for the rest of the day I’d just start crying.”
Generally the most intense pain goes away within minutes – it’s like a fleeting spasm – and women are left with a dull ache for the rest of the day. And as several women have pointed out, it’s much less painful than one possible alternative: childbirth.
The copper IUD paralyses and even decapitates sperm, making egg fertilisation highly unlikely (Credit: BBC/Getty)
In fact, for years doctors thought that the pain of inserting an IUD would only be bearable for women who had already given birth, because their birth canals would be slightly stretched. This had an unfortunate effect: for years, many women didn’t hear about this method from their doctors. We now know that it doesn’t make a lot of difference – women who have already given birth tend to rate their pain as a “level four”, as opposed to a “level six”.
Many doctors are now arguing that all women should be given the option of having a local anaesthetic before insertion, in the hope that this will increase the number of women getting IUDs. Regardless, the popularity of these ingenious, sperm-slaying devices has been increasing steadily since the 2000s. “There’s a big push to recommend IUDs as a first-line option,” says Dweck. Though they’re expensive to buy and insert, over, say, a 10-year lifespan, they can be more cost effective than birth control pills – and health providers have caught on. Who knows – maybe articles about how they exist will soon be redundant.